A Man with Bitemporal Mass: A Rare Manifestation of Epileptic Seizure
Keywords:
Seizure, Epilepsy, Mass, Case ReportAbstract
Introduction: Seizure occurrences are spontaneous and sometimes have no apparent trigger; while it is rarely observed that oral and maxillofacial practices encounter cases presenting epilepsy sporadically. This is a report of a facial mass manifestation after a seizure that is not previously reported.
Case presentation: The presented case is a 27-year-old Caucasian male admitted to the emergency department after a severe tonic-clonic seizure on the same day, with extreme bilateral and symmetric swelling of the buccal and temporal regions. The patient was a known case of chronic end-stage kidney disease and epilepsy. Clinical and imaging studies revealed bilateral subcutaneous soft tissue hypertrophy at the temporal region. The patient’s complaint got improved with conservative treatment after one month.
Conclusion: This case report raises many questions and has provided no answer for the causality of the reported symptom.
Learning points:
- Soft tissue swellings in face are rare; while could be associated with important diagnoses.
- Soft tissue swelling of temporal region of face might happen after seizures and could be diagnosed by non-contrasted CT scans of face.
Declarations:
Conflicts of interest:
None.
Funding:
None.
Authors' contributions:
MF and AH visited the patient at first. MTD, SAA, SRA, and RF participated in drafting the manuscript. All authors had a role in revisions.
Acknowledgments
None.
Ethical considerations
No data that could contribute to the identification of the patient is presented in the paper. The patient signed a consent informed form to participate in this research.
UiEM promotes transparency in Peer-Review to achieve high-quality science. Where reviewers have not given permission of publishing review detail and their identity, the review process is visualized by Microsoft Word version track
changes algorithms. The peer-Review Track change of this manuscript is available here. The file is protected by a password (123123) to protect files from any machine detecting potential plagiarism sources in non peer reviewed files.
---------------------------------------------------------------------------------------------------------------------
Full Text
Epilepsy is a neurological disease that may involve patients of different races, ages, and social occupations (1). The condition affects nearly 70 million people around the world and about 90 percent of these people are found in developing countries. The incidence of this neurological problem is 2.4 million people annually. The median prevalence of epilepsy is 1.54% in rural parts and 1.03% in urban parts (2). This disease has several risk factors including cerebrovascular accidents, congenital anomalies, different types of metabolic diseases, and other less common pathologies. (3).
Buccal swelling is especially a chronic condition that rarely happens acutely. One of the causes of chronic enlargement of buccal region may be occurrence of the lipomas, however, it is not common and accounts for only one-fifth of lipoma cases (4). Furthermore, this swelling may occur due to the reaction to foreign chemical materials such as silicone cosmetic fillers or after the application of braces; however, these two conditions may present with inflammation signs and symptoms (5, 6). Another rare cause of buccal swelling is adenomatoid hyperplasia of minor salivary glands in the buccal mucosa (7). Other causes of buccal swelling may involve infectious diseases such as viral infectious (8). However, there is no case of buccal bulging after epileptic seizures. Here we present a case of soft tissue swelling in the buccal region after an episode of epileptic seizure.
Case presentation
A 27-year-old Caucasian male was referred to the emergency room with acute bilateral and symmetric swelling of the buccal and temporal regions, following a generalized tonic-clonic seizure on the same day. The patient had no complaint of pain in the buccal region and his companions reported no occurrence of trauma to these regions during the epileptic seizure. In the past medical history, the patient was a case of hypertension, as well as end-stage renal disease from 7 years ago, underwent dialysis, and was a case of untreated epilepsy from childhood. The patient’s drug history was comprised of metoprolol 40 mg BID and captopril 25 mg BID. Figure 1 presents the clinical feature of the patient.

Figure 1. Patients’ clinical feature
Upon admission to the emergency department, the patient was alert and oriented but ill and had a blood pressure of 160/80 mmHg, a pulse rate of 65 beats per minute, and a temperature of 36˚C. The O2 saturation was 98% and blood glucose sugar was reported 110 mg/dl using glucometer examination. Physical examination of the patient had nothing positive except for a pale conjunctiva and a bilateral and symmetric soft tissue bulging in the buccal region; however, the skin of swelling the area was intact with no changes and there was no tenderness upon palpation. The neurological examination for pupils’ reactions, deep tendon reflexes, meningeal examinations, and funduscopy were normal. After full physical assessment, a comprehensive laboratory assessment including complete blood cell count, sodium, potassium, blood urea nitrogen, creatinine, calcium, magnesium, blood sugar, PT, PTT, and INR was performed. The laboratory findings showed a low platelet of 90000 with normal PT, PTT, and INR, a urea of 105 mg/dl, and a creatinine of 7.6 mg/dl. Serum LDH (902 U/L) and alkaline phosphatase (1383 U/L) were elevated. The patient then underwent brain and facial CT scan that showed no significant findings except for subcutaneous soft tissue hypertrophy without any pathology of the skin (figure 2). An ENT consult was requested and which resulted in the decision of withholding emergency intervention.
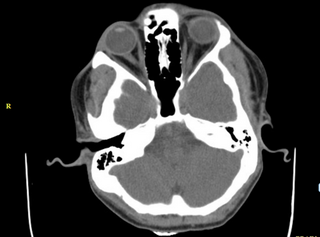
Figure 2. brain and facial CT scan
The patient’s bitemporal swelling got improved with outpatient conservative management after one month. The patient had no further compliant during the follow-ups.
Discussion
The anatomic borders of the buccal region consist of the zygomatic bone, mandible, masseter muscle, and buccinator muscle. The region is majorly filled with Bichat’s fat pad and buccal fat. Other anatomical parts are regional lymph nodes and parotid gland. Stensen duct, the facial motor nerves crossing the region and terminal branches of the second trigeminal nerve run through this region beside arterial and venous vessels. The bulging in the buccal region may be due to the overgrowth or enlargement of any of the above mentioned anatomical parts (9).
This buccal swelling may occur due to several predisposing factors. It may occur due to the growth and enlargement of soft tissue beneath the cheek in the presence of tumors such as lipomas, solitary fibrous tumors, pleomorphic adenoma, epidermoid cyst, and adenomatoid hyperplasia of minor salivary glands (9, 10). Brown et al reported a 11-year old boy with buccal swelling due to irritant contact dermatitis caused by applying orthodontic braces (5). Another case report by Dereci et al reported a 48 year old male presented with painless buccal bulging on the left cheek with a bluish mass inside the mucosa. The pathologic assessment revealed adenomatoid hyperplasia of minor salivary glands which is a rare condition (7). Thanthoni et al. reported a 53-year old man with chronic swelling of the buccal region and was diagnosed with pathology as a lipoma mass (4). Martínez et al presented another case of buccal swelling who was a 23 year old female with painless swelling of the cheek during the past year. The biopsy revealed a brownish mass with pathologic assessment of secretory carcinoma of the salivary gland (10).
Other pathologies that cause buccal bulging are infectious diseases such as parotiditis or lymphadenopathies in the region (11). However, the presented case in this study had no signs of inflammation or skin changes. Also, the bulging was symmetrical and bilateral on both cheeks. Furthermore, the buccal swelling occurred just a little after the epileptic seizure in an acute manner. Thus, it seems the problem may not be due to tumor growth or infections. Furthermore, as the patient used no antiepileptic drug, the soft tissue bulging cannot be attributed to the side effect of the drugs. Also, the patient had no history of trauma during seizure. It seems that the condition is caused due to some events during seizure such as bruxism, yet it may not fully address the temporal region swelling. Furthur investigation and reporting of similar cases may help clarify the etiology or they may not have an effect on diagnosis. It seems that this condition is a rare presentation or complication of an epileptic seizure.
Conclusion:This unique case raised questions about the etiology of this bitemporal swelling while has provided no answer for the causality of the reported symptom.
References
1. Singh A, Trevick S. The epidemiology of global epilepsy. Neurologic clinics. 2016;34(4):837-47.
2. Ngugi AK, Bottomley C, Kleinschmidt I, Sander JW, Newton CR. Estimation of the burden of active and life‐time epilepsy: a meta‐analytic approach. Epilepsia. 2010;51(5):883-90.
3. Behr C, Goltzene M, Kosmalski G, Hirsch E, Ryvlin P. Epidemiology of epilepsy. Revue neurologique. 2016;172(1):27-36.
4. Thanthoni M, Sathasivasubramanian S, Warrier A. Persistent Buccal Swelling: Diagnostic Dilemma. Cureus. 2018;10(12).
5. Brown J. BUCCAL SWELLING AFTER APPLICATION OF BRACES. Annals of Allergy, Asthma & Immunology. 2018;121(5):S121.
6. Mandel L, Addison S, Clark M. Buccal reaction to silicone cosmetic filler. The Journal of the American Dental Association. 2010;141(2):162-6.
7. Dereci Ö, Çimen E. Adenomatoid hyperplasia of the minor salivary glands on the buccal mucosa: A rare case report. International journal of surgery case reports. 2014;5(5):274-6.
8. Conversano E, Udina C, Cozzi G, Dal Bo S, Marchetti F, Barbi E. IMAGES IN EMERGENCY MEDICINE DIAGNOSIS: Acute mastoiditis associated with temporal osteomyositis with intra-and extracranial abscess. MOSBY-ELSEVIER 360 PARK AVENUE SOUTH, NEW YORK, NY 10010-1710 USA; 2019.
9. Franzen A, Glitzki S, Coordes A. How to Manage a Buccal Space Mass–A Case Series. Austin Head Neck Oncol. 2018;2(1):1008.
10. Martínez R, Marín C, Niklander S, Marshall M, González-Arriagada WA. Exophytic swelling of the buccal mucosa in a young female patient. Oral surgery, oral medicine, oral pathology and oral radiology. 2019;127(4):267-71.
11. Cataño J, Robledo J. Tuberculous Lymphadenitis and Parotitis. Microbiology spectrum. 2016;4(6).
Downloads
Additional Files
Published
How to Cite
Issue
Section
License
Copyright (c) 2022 Updates in Emergency Medicine

This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

